- Okay, so the text book definition for place theory is this: The place theory of pitch perception proposes that pitch is determined by the place of maximum excitation on the basilar membrane.
does this mean that it is the place/location on the basilar membrane where the sound actually makes the membrane vibrate?
Basically yes - actually it makes the membrane vibrate all over, but there's only one place that it vibrates the most.
- Is "chroma" referring to just the single musical note or the string of notes eg. A1 to G1 on the tone helix. or just A1, B1... signally?
Chroma refers to all kinds of a particular note. A low-frequency A (A1) sounds like a similar tone to a high-frequency A (say, A4 or A5). So even though they're different frequencies (the A5 is higher frequency than the A1), they sound similar, and we say they have the same chroma.
- I bumped my arm and so it hurts when I touch it. I understand that it is rapidly adapting because it only hurts when my finger is first pushing the skin. Is it the mechano receptors or the nociceptors or both that are telling me 'ouch that hurts!?"
Well, it's really both, but the nociceptors (the free nerve endings in your skin) were probably damaged, starting the perception of pain when they're stimulated (that is, when you touch your arm). Pain perception is pretty complicated, but if you look in your textbook (or even online) under something called "gate control theory," you can see how complicated it is. The short answer is that both regular mechanoreceptors and nociceptors play a role in pain perception - one of the reasons why rubbing something shortly after it's been hurt can make the pain go away.
- Is the reason that 1000hz sounds louder than 100hz on a certain point in the equal loudness contour because 1000hz is below the hearing threshold?
Not exactly. whenever you talk about the loudness of a sound, you have to talk about both frequency and amplitude. The frequency is in terms of "hertz" and the amplitude is in terms of "decibels." The more decibels (db), the higher the amplitude. So a 1000 hz tone played at 10 db will sound quieter than a 100 hz tone played at 60 db. At the same time, a 100 hz tone played 60 db will sound quieter than a 1000 hz tone played at 60 db (note that the curve at 100hz, 60 db is lower than the curve at 1000 hz, 60 db). Uf you play both tones at (say) 20 db, then the 1000 hz tone will be audible, but you won't even hear the 100 hz tone because that will be below your threshold.
- While looking at a interaural phase difference graph does the first point in the cycle always represent hitting the left ear then the next point it hits the right? How can one tell which ear it hits first by looking at the graph is my question.
You can't - it's not on the graph I showed in class. The only way you could tell is if I labeled 'em for you.
- Why do nearby sounds change their location faster than distant sounds?
It's a geometry thing. Think about the angle something traces out relative to you if it moves 5 feet, and is only 2 feet away from you (it's a large angle) - but think about the angle something traces at a longer distance - say, it moves 5 feet, but is 50 feet away from you (small angle). It might help to actually sit down with some rulers (actually just one ruler should work. :-) and try a couple examples.
- I was wondering if K is constant, does that mean that the criteria is K?
I'm asking because I'm thinking that in an experiment that is a constant? Isn't it?
K the constant is not the same thing as the criterion. (You are right that in a signal detection experiment, however, we generally assume the criterion doesn't change.)
K is called a "constant" because it is a mathematical constant, that is, for any particular type of detection task, and for a given person, it should be the same value (which you have to determine experimentally). K is really meaningful in finding D's for difference thresholds.
The criterion is really not about D's, but rather about your bias to say "yes, I saw the signal" or "no, I didn't see the signal."
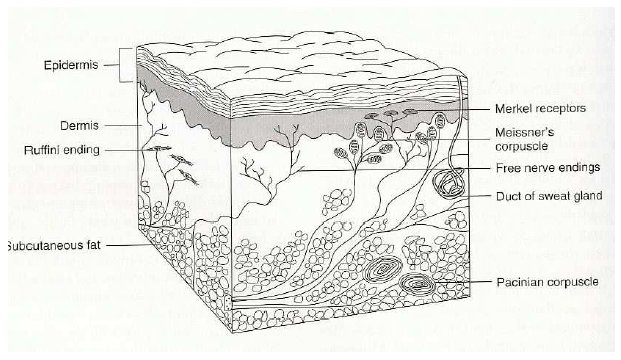
- Can you show a grapic (I know it would be somewhat gruesome) of a real nociceptor?
It's actually not too bad. Here's a diagram of a section of the skin which includes all the mechanoreceptors (the ones labeled "meissner's corpuscles", "ruffini endings", "merkel receptors", and "pacinian corpuscles"), and nociceptors (the ones labeled "free nerve endings"). It's actually a little more complicated than that since there are multiple types of nociceptor, depending on the stimulus to which the nerve responds. For example, if a nociceptor responds to excess heat or cold, it's a thermal nociceptor, whereas if it responds to acids, it's a chemical nociceptor. It's even more complicated, because nociceptors fire at different speeds (some fast, some slow), so pain often comes in two phases (one immediate, one longer-lasting), and that second phase can be trained to be not-entirely unpleasant (why some people like spicy foods, or why you sometimes want to do something like poke at a bruise while it should be healing).
- Are there nociceptors in eg. the brain, bones, musles, body organs?
There are no nociceptors in the brain (so you can have brain surgery with only a local anasthetic for your skin, and you won't feel them poking around it your cerebral cortex). You do have nociceptors in your intestines and bladder, various other internal organs, and in your muscles and joints - basically you have 'em where you feel pain.